AUTHORS
Amnuayporn Apiraksakorn, MD, MMEd, CHSE, LLB, BPH 1; Kittisak Wangsataporn, MD2; Suphot Chattinnakorn, MD2; Wanna Ardonk, MD3; Wasana Hongkan, MD4; Tirachat Sewatanon, MD5; Adisak Tanpun, MD2; Seksun Sribooncharoenchai, MD4
1Khon Kaen Medical Education Center, Khon Kaen, Thailand
2Prapokklao Medical Education Center, Chanthaburi, Thailand
3Buddhachinaraj Medical Education Center, Phitsanulok, Thailand
4Chonburi Medical Education Center, Chonburi, Thailand
5Maharat Nakorn Ratchasima Medical Education Center, Nakorn Ratchasima, Thailand
Corresponding Author
Amnuayporn Apiraksakorn, a.apiraksakorn@cpird.in.th
Conflict of interest statement
The authors have no conflicts of interest to declare.
Funding statement
This research received a research grant from the Bureau of Medical Doctor and Health Care Professional Production and Development, Ministry of Public Health, Thailand.
Acknowledgement
The authors would like to thank all medical education centers for all the hard work and contributions to this project.
Appendix A
Current Practice and Needs Assessment of SBME in MEC Questionnaire: https://forms.gle/DFQtYQWV1e2hJBZ7A
Please cite this article as: Apiraksakorn, A., Wangsataporn, K., Chattinnakorn, S., Ardonk, W., Hongkan, W., Sewatanon, T., Tanpun, A., & Sribooncharoenchai, S. (2026). Current practice of simulation-based medical education in medical education centers in Thailand. Simulation Technology & Operations Resource Magazine, 5(1), 13-21. ISSN: 3070-3506.
SUMMARY
Introduction: Simulation-based medical education (SBME) has become an essential component of medical training, offering learners the opportunity to acquire and refine clinical skills in a controlled and safe environment. In 2020, the Thai Medical Council (TMC) revised the procedural skill requirements for the national medical licensing examination, emphasizing competency-based training and assessment. This study aims to evaluate the current SBME practices across Medical Education Centers (MECs) in Thailand in accordance with the updated TMC criteria.
Methods: A descriptive cross-sectional study was conducted across all MECs in 2024 in Thailand. Data were collected through an online, self-administered questionnaire covering institutional demographics, policies, staffing, facilities, equipment, and the implementation of procedural competencies based on the 2020 TMC guidelines. Descriptive statistics were used to analyze and report the findings.
Results: All 35 MECs (100% response rate) completed the survey, comprising 16 small, 10 medium, and 9 large centers. Of these, 30 MECs (86%) reported having established SBME policies, staff, teaching schedules, simulation center, mannequins, and training equipment. However, only 24 centers (69%) had a simulated patient (SP) bank, and 15 centers (43%) had formal SP training programs. A total of 274 instructors (5%) had received prior training in simulation-based teaching, and only 16 simulation technicians were employed across all centers. The majority of MECs incorporated SBME into instruction for core clinical competencies, with 29 centers (83%) utilizing it for both formative and summative assessments. All centers reported training in key procedures such as basic and advanced life support, endotracheal intubation, defibrillation, intravenous access, and intercostal drainage. Conversely, procedures like nail removal, skin traction, and strengthening exercises were inconsistently taught across institutions.
Conclusions: Evaluating the current practice of SBME across Thailand’s MECs provides valuable insights into areas needing improvement. Enhancing SBME resources, standardizing training programs, and expanding faculty development are critical steps toward strengthening the quality of medical education and improving clinical preparedness among future healthcare professionals.
INTRODUCTION
Simulation-based Medical Education (SBME) is widely accepted in the training of medical students and has been shown to enhance learners’ development in both simulated and clinical settings (Griswold-Theodorson et al., 2015; McGaghie et al., 2011; McInerney et al., 2022; Steinemann et al., 2011; Stone et al., 2014). Simulation supports the improvement of learners’ knowledge, procedural skills, and non-technical skills, including cognitive processes, communication and social interaction, teamwork, and decision-making (Cook et al., 2012; Lamé & Dixon-Woods, 2018; Motola et al., 2013; Paige et al., 2018). At present, SBME is utilized in Thailand for teaching medical students both in medical schools and in medical education centers (MECs) under the Bureau of Medical Doctor and Health Care Professional Production and Development (MPHD). The national survey conducted in 2019-2020 included the SBME in 15 medical schools in Thailand according to the first edition (2002) Thai Medical Council (TMC) criteria (Boonmak et al., 2022). Of these, 6/15 medical schools (40%) did not have simulation centers, and the implementation of SBME in teaching procedural skills ranged from 42% to 99% of the 46 procedures. However, there is a lack of published data examining the current practice in SBME implementation within MECs, which serve as teaching hospitals affiliated with medical schools and operate under distinct contextual conditions. Additionally, the Thai Medical Council revised its competency-based licensing examination criteria in the second edition (2020), reducing the number of required procedural skills from 46 to 30 procedures, and mandating the assessment of 15 procedural skills. To date, there have been no published studies reporting on these developments. This study aims to evaluate the current SBME practices across Medical Education Centers in Thailand in accordance with the updated TMC criteria.
METHODS
A descriptive cross-sectional survey study was performed in all 35 MECs under MPHD, which currently have clinical year medical students in 2024 in Thailand. An online self-administered questionnaire was used to collect data, including demographic data of the simulation center, policies, staffing, facility resources, equipment, and the current practice using SBME in teaching, learning, and assessment of competencies as outlined by the 2020 TMC criteria. The questionnaire is available in Appendix A. The respondents of the online questionnaire were representatives of the MECs, including directors, deputy directors, instructors, or educators involved with SBME. The data were reported in accordance with STROBE guidelines (Von Elm et al., 2007). The categorical data were presented as percentages and frequencies and analyzed using descriptive statistics. Chanthaburi Research Ethics Committee /region 6 has approved this study (COA no. 073/67).
RESULTS
Demographic Data
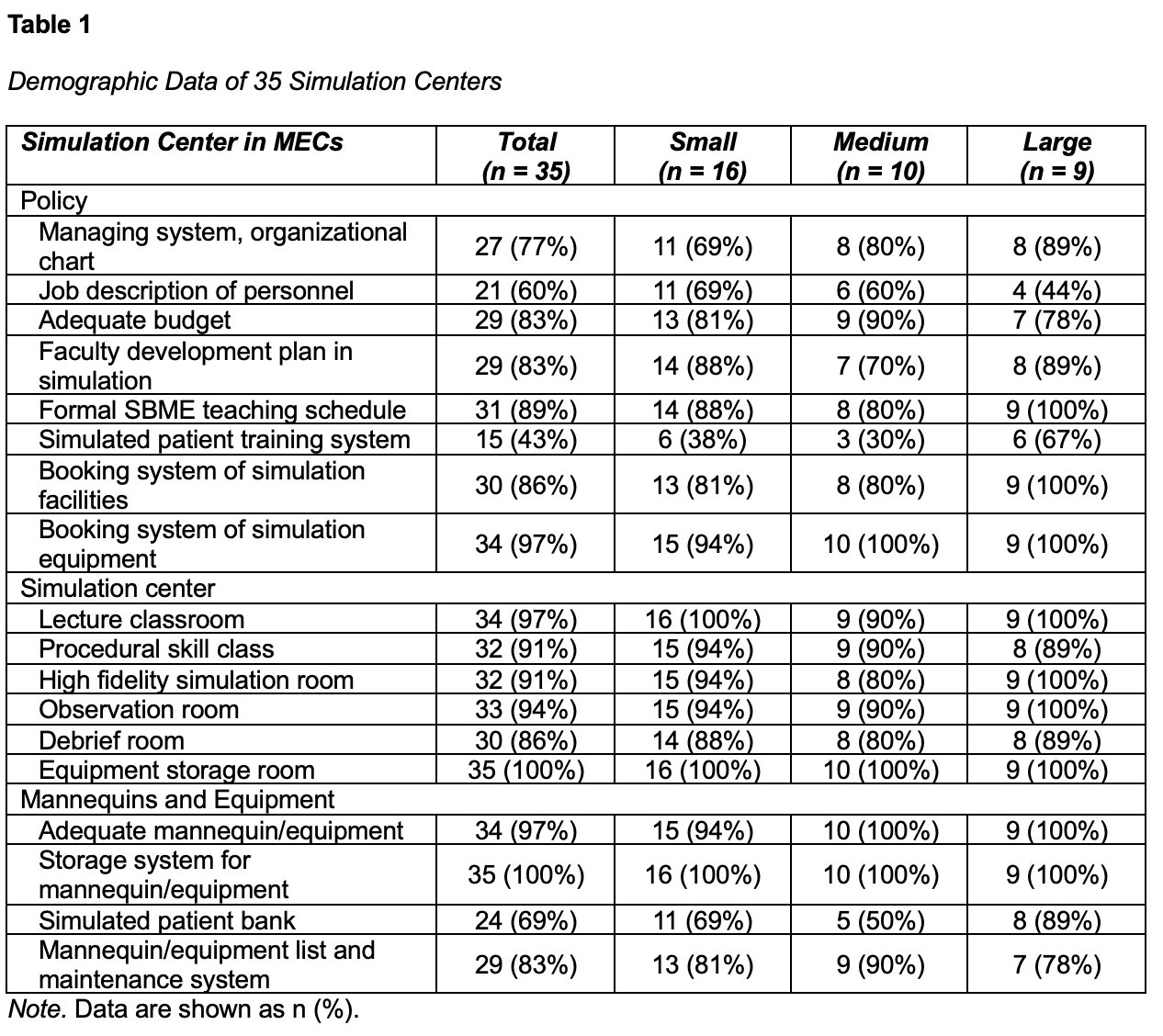
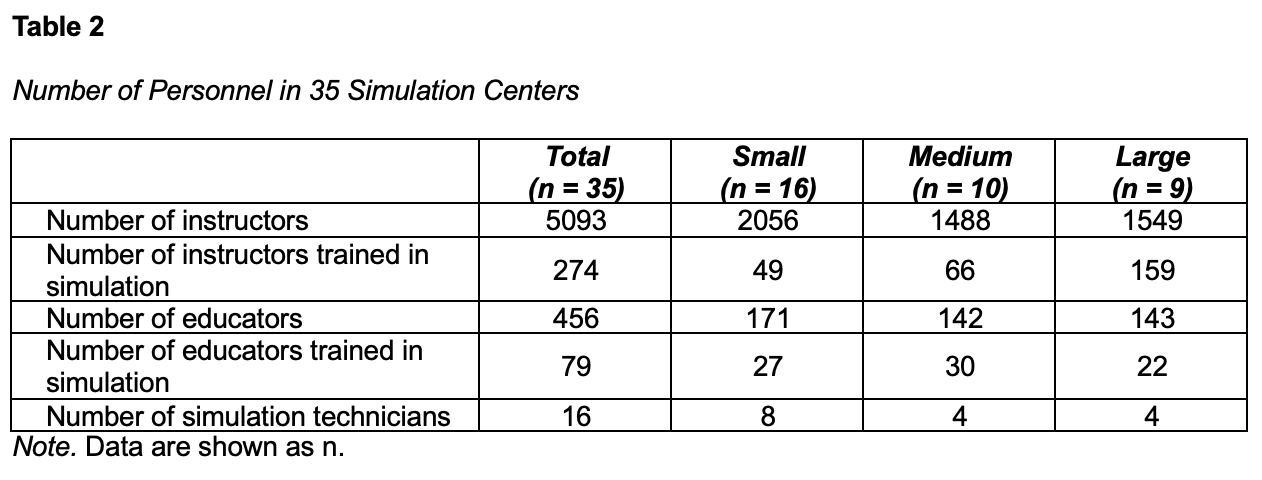
Thirty-five MEC representatives (100% response rate) responded to the online questionnaire, including 16 small, 10 medium, and 9 large-size centers (Table 1). Thirty MECs (86%) have established clear policies regarding simulation staffing, faculty development plan, SBME teaching schedule, simulation center layout, mannequins, and equipment. However, only 24 MECs (69%) have simulated patient (SP) banks, and 15 MECs (43%) have SP training programs. Across all MEC personnel, only 274 of the 5093 instructors and 79 of the 456 educators had previous simulation training. There were only 16 simulation technicians currently working across all 35 simulation centers, including 8 in small, 4 in medium, and 4 in large-sized MECs (Table 2).
Current Practice of SBME in MECs
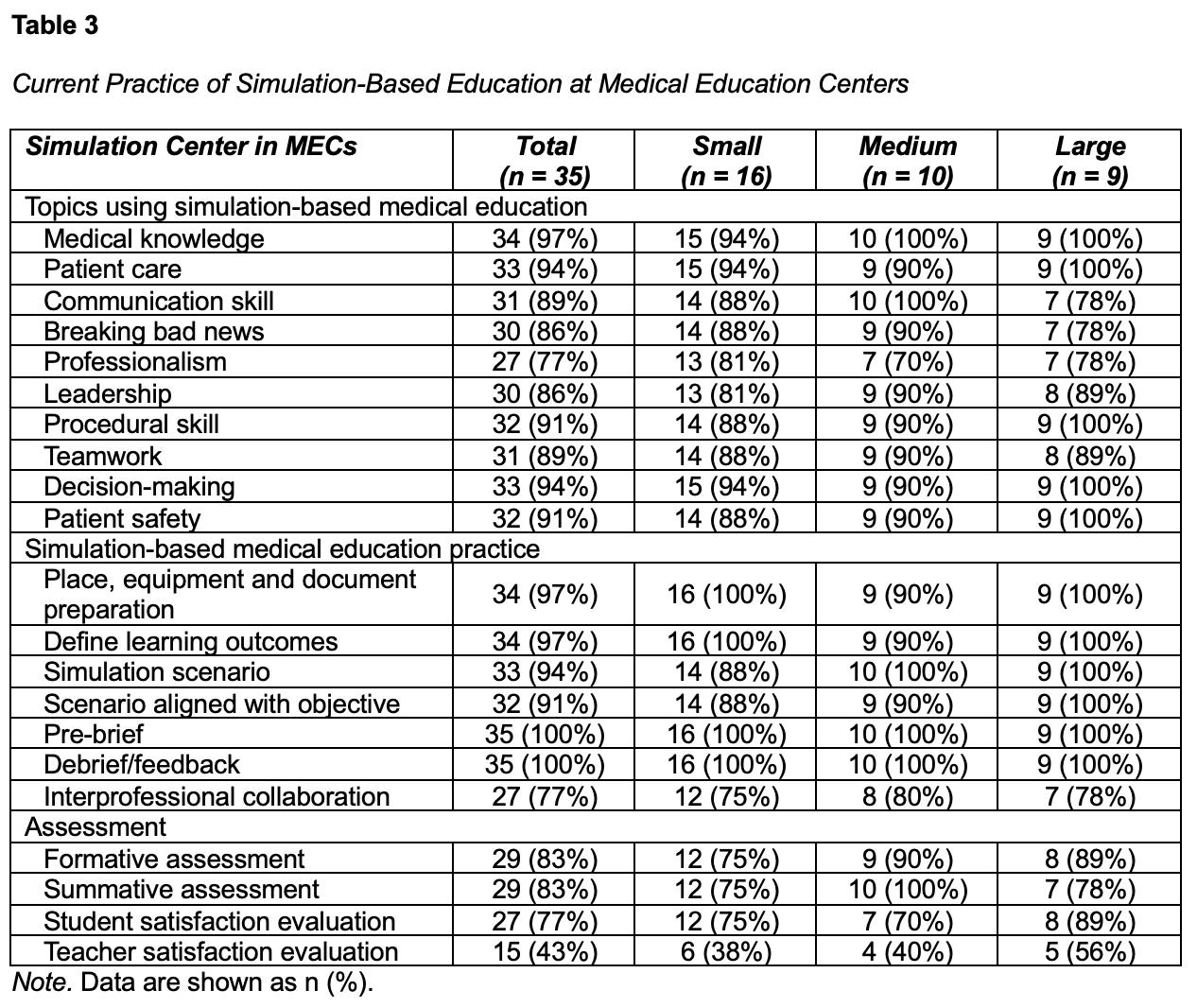
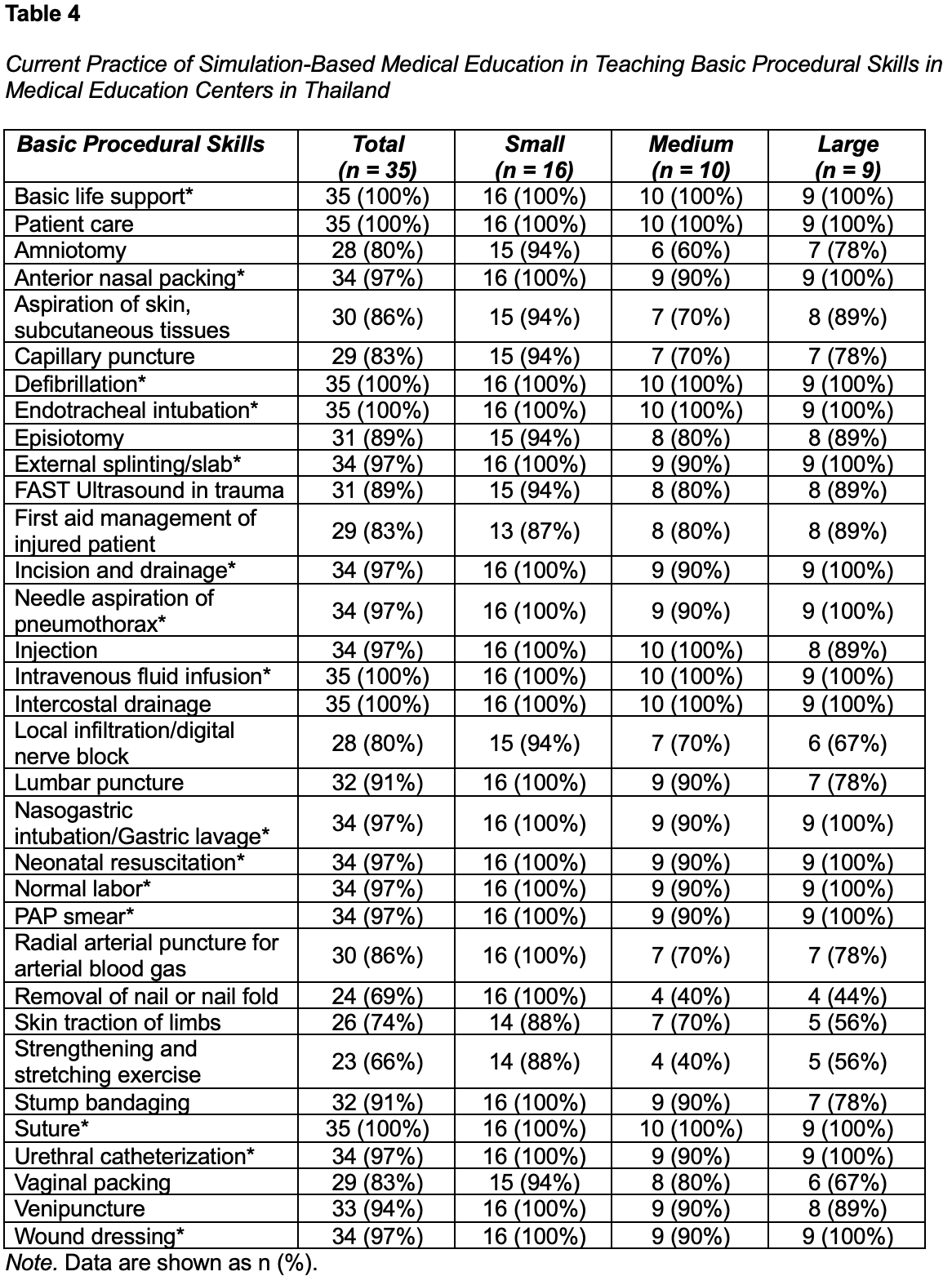
Most MECs (77-97%) utilized SBME for teaching essential competencies, such as medical knowledge, patient care, communication, professionalism, procedural skills, teamwork, decision-making, and patient safety (Table 3). Scenario-based training often involved collaboration with other healthcare professions across 27 MECs (77%). Twenty-nine MECs (83%) reported using SBME in both formative and summative assessments. Twenty-seven MECs (77%) and 15 MECs (43%) reported implementing student and teacher satisfaction evaluation in SBME, respectively. All MECs (100%) reported teaching basic and advanced life support, endotracheal intubation, defibrillation, intravenous access, and intercostal drainage (Table 4). However, certain procedures, such as nail removal, skin traction, and strengthening exercises, were not consistently covered across all centers. SBME was predominantly teaching at both undergraduate (95%) and postgraduate (87%) levels.
DISCUSSION
This study represents the current nationwide practice of simulation-based medical education across all Medical Education Centers in Thailand following the Thai Medical Council’s 2020 competency revisions. The findings indicate that, although most centers have established policies, personnel, and facilities to support SBME, certain procedural skills require more comprehensive coverage to ensure students achieve the required competencies prior to graduation. Challenges related to SP banks, SP training systems, and training instructors and simulation technicians underscore the need for sustained institutional and national support for SBME.
This investigation was conducted within the context of the 2020 revision of the Medical Council of Thailand’s licensing examination criteria. Compared with previous research, such as the Boonmak et al. (2020) study of 15 medical schools (only nine of which had simulation centers), this study provides a more comprehensive and updated perspective on the integration of simulation in clinical education. The findings demonstrate that most simulation centers are now equipped with adequate policies, personnel, facilities, and equipment to support simulation-based instruction, contrasting with earlier studies that reported insufficient funding (Bouthors et al., 2022; Elendu et al., 2024; Forristal et al., 2020; Lawaetz et al., 2023; Sawaya et al., 2021; Seethamraju et al., 2021) and resource-related barriers (Campbell et al., 2022; Lawaetz et al., 2023; Sawaya et al., 2021; Tranel et al., 2021). Nonetheless, small- and medium-sized centers frequently lack structured registries and formal training programs for standardized patients, indicating a need for system development. This is consistent with prior reports of technician shortages in 93% of Thai medical schools (Boonmak et al., 2022). In addition, a nationwide shortage of trained simulation educators (Campbell et al., 2022; Lawaetz et al., 2023; Sawaya et al., 2021; Tranel et al., 2021) and technicians persists (Ismail et al., 2024; Tellefson et al., 2025). The effectiveness of SBME relies on multidisciplinary teams, with simulation technicians playing a critical supporting role (Ismail et al., 2024; Tellefson et al., 2025). In response, Thailand has initiated the development of professional and qualification standards for simulation technicians within the health services sector to define nationally and internationally recognized competency levels, which is expected to increase interest in this profession.
SBME is now widely implemented across curricula in accordance with TMC standards, including the assessment of 15 procedural skills. This aligns with global evidence that simulation enhances both technical and non-technical competencies, such as clinical reasoning, communication, teamwork, and decision-making (Cook et al., 2012; Lamé & Dixon-Woods, 2018; Motola et al., 2013; Paige et al., 2018). Simulation-based learning has also been shown to improve procedural skill confidence (Nestel et al., 2011) and prevent skill decay (Higgins et al., 2020). All Medical Council competency domains—medical knowledge, patient care, communication, professionalism, leadership, procedural skills, teamwork, decision-making, and patient safety—are addressed through simulation (McGaghie et al., 2011). However, gaps remain in the teaching of several basic procedural skills required for graduation, including nail or nail fold removal, skin traction of limbs, and strengthening or stretching exercises. These deficiencies highlight priority areas for curriculum enhancement and further investment in simulation-based training across Thailand’s medical education system.
A major strength of this study is that it represents the first nationwide assessment of SBME practices across all 35 medical simulation centers under the Ministry of Public Health using the updated 2020 TMC criteria. A key limitation is the reliance on self-reported data regarding SBME availability. The quality of SBME should therefore be continuously monitored and standardized to meet TMC requirements. Although the findings are most directly applicable to MEC settings, which differ from university-based medical schools, they provide important insights for national planning. Future studies should include a national survey combined with on-site evaluations to ensure quality and guide systematic improvement of SBME in all Thai medical simulation centers.
CONCLUSION
Evaluating the current practice of SBME across Thailand’s MECs provides valuable insights into areas needing improvement. Enhancing SBME resources, standardizing training programs, and expanding faculty development are critical steps toward strengthening the quality of medical education and improving clinical preparedness among future healthcare professionals.
REFERENCES
Boonmak, P., Suraseranivongse, S., Pattaravit, N., Boonmak, S., Jirativanont, T., Lertbunnaphong, T., Arora, R., Watcharotayangul, J., Imsuwan, I., Kwangwaropas, P., & Wittayachamnankul, B. (2022). Simulation-based medical education in Thailand: a cross-sectional online national survey. BMC Medical Education, 22(1), 298. https://doi.org/10.1186/s12909-022-03369-9
Bouthors, C., Dagneaux, L., Boisgard, S., De Loubresse, C. G., Benhamou, D., & Court, C. (2022). Procedural simulation training in orthopaedics and traumatology: Nationwide survey among surgeon educators and residents in France. Orthopaedics & Traumatology Surgery & Research, 108(8), 103347. https://doi.org/10.1016/j.otsr.2022.103347
Campbell, K. K., Wong, K. E., Kerchberger, A. M., Lysikowski, J., Scott, D. J., & Sulistio, M. S. (2022). Simulation-Based education in US Undergraduate medical education. Simulation in Healthcare the Journal of the Society for Simulation in Healthcare, 18(6), 359–366. https://doi.org/10.1097/sih.0000000000000705
Cook, D. A., Hamstra, S. J., Brydges, R., Zendejas, B., Szostek, J. H., Wang, A. T., Erwin, P. J., & Hatala, R. (2012). Comparative effectiveness of instructional design features in simulation-based education: Systematic review and meta-analysis. Medical Teacher, 35(1), e867–e898. https://doi.org/10.3109/0142159x.2012.714886
Elendu, C., Amaechi, D. C., Okatta, A. U., Amaechi, E. C., Elendu, T. C., Ezeh, C. P., & Elendu, I. D. (2024). The impact of simulation-based training in medical education: A review. Medicine, 103(27), e38813. https://doi.org/10.1097/md.0000000000038813
Forristal, C., Russell, E., McColl, T., Petrosoniak, A., Thoma, B., Caners, K., Mastoras, G., Szulewski, A., Chaplin, T., Huffman, J., Woolfrey, K., Dakin, C., & Hall, A. K. (2020). Simulation in the continuing professional development of academic emergency physicians. Simulation in Healthcare the Journal of the Society for Simulation in Healthcare, 16(4), 246–253. https://doi.org/10.1097/sih.0000000000000482
Griswold-Theodorson, S., Ponnuru, S., Dong, C., Szyld, D., Reed, T., & McGaghie, W. C. (2015). Beyond the simulation laboratory. Academic Medicine, 90(11), 1553–1560. https://doi.org/10.1097/acm.0000000000000938
Higgins, M., Madan, C., & Patel, R. (2020). Development and decay of procedural skills in surgery: A systematic review of the effectiveness of simulation-based medical education interventions. The Surgeon, 19(4), e67–e77. https://doi.org/10.1016/j.surge.2020.07.013
Ismail, F. W., Ajani, K., Baqir, S. M., Nadeem, A., Qureshi, R., & Petrucka, P. (2024). Challenges and opportunities in the uptake of simulation in healthcare education in the developing world: a scoping review. MedEdPublish, 14, 38. https://doi.org/10.12688/mep.20271.1
Lamé, G., & Dixon-Woods, M. (2018). Using clinical simulation to study how to improve quality and safety in healthcare. BMJ Simulation & Technology Enhanced Learning, 6(2), 87–94. https://doi.org/10.1136/bmjstel-2018-000370
McGaghie, W. C., Draycott, T. J., Dunn, W. F., Lopez, C. M., & Stefanidis, D. (2011). Evaluating the impact of simulation on translational patient outcomes. The Journal of the Society for Simulation in Healthcare, 6(7), S42–S47. https://doi.org/10.1097/sih.0b013e318222fde9
McInerney, N., Nally, D., Khan, M., Heneghan, H., & Cahill, R. (2022). Performance effects of simulation training for medical students – a systematic review. GMS Journal of Medical Education, 39(5), Doc51. https://doi.org/10.3205/zma001572
Motola, I., Devine, L. A., Chung, H. S., Sullivan, J. E., & Issenberg, S. B. (2013). Simulation in healthcare education: A best evidence practical guide. AMEE Guide No. 82. Medical Teacher, 35(10), e1511–e1530. https://doi.org/10.3109/0142159x.2013.818632
Nestel, D., Groom, J., Eikeland-Husebø, S., & O’Donnell, J. M. (2011). Simulation for learning and teaching procedural skills. The Journal of the Society for Simulation in Healthcare, 6(7), S10–S13. https://doi.org/10.1097/sih.0b013e318227ce96
Paige, J. T., Fairbanks, R. J. T., & Gaba, D. M. (2018). Priorities related to improving healthcare safety through simulation. Simulation in Healthcare the Journal of the Society for Simulation in Healthcare, 13(3S), S41–S50. https://doi.org/10.1097/sih.0000000000000295
Sawaya, R. D., Mrad, S., Rajha, E., Saleh, R., & Rice, J. (2021). Simulation-based curriculum development: lessons learnt in Global Health education. BMC Medical Education, 21(1), 33. https://doi.org/10.1186/s12909-020-02430-9
Seethamraju, R. R., Stone, K. P., & Shepherd, M. (2021). Factors affecting implementation of Simulation-Based Education after faculty training in a Low-Resource setting. Simulation in Healthcare the Journal of the Society for Simulation in Healthcare, 17(1), e113–e121. https://doi.org/10.1097/sih.0000000000000549
Steinemann, S., Berg, B., Skinner, A., DiTulio, A., Anzelon, K., Terada, K., Oliver, C., Ho, H. C., & Speck, C. (2011). In situ, multidisciplinary, Simulation-Based teamwork training improves early trauma care. Journal of Surgical Education, 68(6), 472–477. https://doi.org/10.1016/j.jsurg.2011.05.009
Stone, K., Reid, J., Caglar, D., Christensen, A., Strelitz, B., Zhou, L., & Quan, L. (2014). Increasing pediatric resident simulated resuscitation performance: A standardized simulation-based curriculum. Resuscitation, 85(8), 1099–1105. https://doi.org/10.1016/j.resuscitation.2014.05.005
Tellefson, F., Dawson, K., Zhang, N. M., Dickie, R., Coyte, B., & Jacob, A. (2025). The role and impact of the simulation technician in health science higher education: A scoping review. Clinical Simulation in Nursing, 100, 101695. https://doi.org/10.1016/j.ecns.2025.101695
Tranel, G. E., Johanneck, M. D., Thompson, R. J., & Campbell, K. K. (2021). Results of a nationwide descriptive survey on simulation center operations. Clinical Simulation in Nursing, 53, 32–41. https://doi.org/10.1016/j.ecns.2020.12.008
Von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., & Vandenbroucke, J. P. (2007). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. The Lancet, 370(9596), 1453–1457. https://doi.org/10.1016/s0140-6736(07)61602-x