A Hybrid Approach Using Digital Tools and High-Fidelity Simulation
AUTHORS
Nathan Stewart, BSN, RN, CCRN1; Jennifer Fuka, BSN, RN, NPD-BC, CCRN-CSC1; Cornelia Carley, BSN, RN, CCRN, CMSRN1; Kirk Atkinson, CHSOS1; Anthony Austin, CHSOS1; Jeanne Carey, MEd, RN, CHSE-A1
1UT Southwestern Medical Center, Dallas, TX
Corresponding Author
Nathan Stewart, Nathan.stewart@utsouthwestern.edu
Conflict of interest statement
The authors have no conflicts of interest to declare.
Please cite this article as: Stewart, N., Fuka, J., Carley, C., Atkinson, K., Austin, A., & Carey, J. (2026). Reimaging Emergency Resternotomy Education: A Hybrid Approach Using Digital Tools and High-Fidelity Simulation. Simulation Technology & Operations Resource Magazine, 5(1), 6-12. ISSN: 3070-3506.
SUMMARY
Emergency resternotomies in the Cardiovascular Intensive Care Unit (CVICU) are high-stakes events requiring rapid response and precise role execution (Tsiouris et al., 2024). Previously, at our institution, emergency resternotomy training consisted of a didactic session and a simulation. Although the simulation session offered an opportunity for teams to practice chest reopening procedures, the standard manikin lacked anatomical realism.
While this training was helpful, staff feedback and post-simulation evaluations revealed ongoing gaps in role clarity, procedural confidence, and knowledge retention. In response, educators collaborated with the simulation center to develop a high-fidelity open chest manikin featuring realistic thoracic anatomy (Hill et al., 2023). Additionally, an Open Chest Digital Library was created to serve as pre-simulation work, followed by concise, role-based training videos (Stewart et al., 2024). This hybrid approach was integrated into the existing training model, aligning digital learning, structured classroom instruction, and realistic simulation. Early feedback demonstrated improved learner confidence, higher engagement, and increased procedural accuracy during drills. This session will explore the development and implementation of the upgraded training program, challenges encountered, and how combining digital education with high-fidelity simulation can better prepare teams for rare but critical clinical events.
INTRODUCTION
Open chest emergencies, including emergency resternotomy and internal cardiac massage, demand rapid, role-specific action. Despite scheduled didactic classes and simulations, inconsistencies in role clarity and team response persisted among critical care nurses and support staff. Existing training relied on a standard manikin with simulated actions, limiting the realism and practice of procedural steps. The goal of this initiative was to enhance the training environment by pairing technology-enabled education with a high-fidelity physical model. This approach reflects current best practices in simulation-based education: layering digital prebriefing, real-time role reinforcement, and realistic scenario enactment.
For the purposes of this manuscript, learners are defined as bedside cardiovascular intensive care unit (CVICU) registered nurses and advanced practice providers participating in the training. Educators include nurse professional development specialists and simulation center staff responsible for curriculum design, facilitation, and debriefing. Nursing leadership refers to unit-based clinical leaders who supported implementation but did not participate as learners. This manuscript details the systematic redesign of the training program, its components, and early outcomes.
METHODS
Needs Assessment and Gap Identification
Feedback from post-simulation surveys completed by CVICU registered nurses and advanced practice providers, as well as unit-based incident debriefs facilitated by nurse educators and nursing leadership, highlighted gaps in the previous training. This includes recurring gaps in knowledge retention, procedural execution, and role assignment, particularly during code events involving open chest scenarios. In response, a multidisciplinary team consisting of nurse educators, simulation specialists, and nursing leaders convened to evaluate training barriers and redesign the approach.
Development of the Open Chest Digital Library
To prepare learners prior to entering the simulation lab, a series of concise, high-yield educational videos was created. Each video was filmed using clinical-grade equipment, professionally edited for clarity, and reviewed by educators and nursing leadership to ensure clinical accuracy and consistency with institutional protocols. These videos, housed in an accessible digital library, covered key topics such as:
What is Cardiac Tamponade and the 6 Roles of the Open Chest Protocol
The Emergency Resternotomy Cart
Internal Defibrillation
How to Get Sterile
The Open Chest Simulation Walkthrough
Code Documentation Related to the Open Chest Simulation
These modules were developed to promote visual proficiency (Stewart et al., 2024), enhance role comprehension, and support just-in-time learning principles.
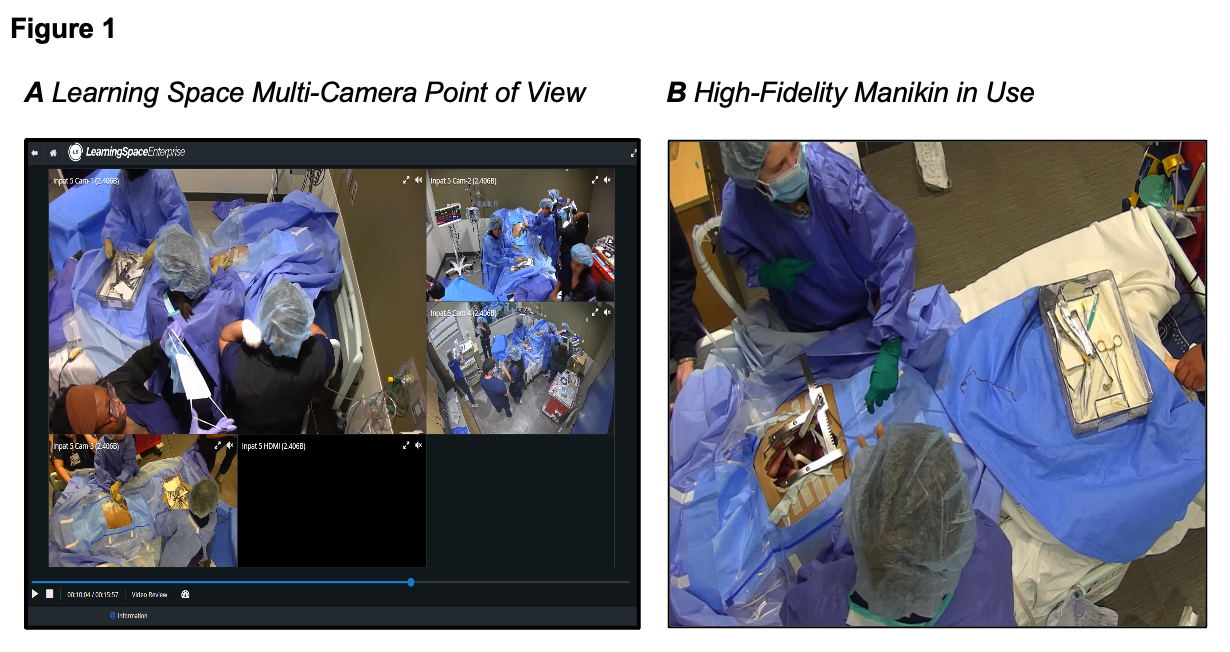
High-Fidelity Manikin Design
To develop the high-fidelity open chest manikin, educators and simulation center specialists identified essential features that would replicate an emergency resternotomy scenario with anatomical realism. The team sourced a thoracic cavity model from Strategic Operations, which became the foundation of the build. This model costs around $60,000 and is a one-time cost. Guided by clinical expertise, a midsternal incision was sawed into the model’s sternum, and copper wires were applied to approximate closure. This simulated the reality of post-operative sternotomy wiring.
A silicone heart was positioned strategically within the thoracic cavity so that it was accessible once the sternum was opened using a retractor. The thoracic model was mounted over a standard manikin, and a realistic skin layer was applied over the chest. A six-inch mid-sternal incision was made into the skin layer, then sealed using an adhesive designed to mimic Dermabond.
Integration of Revised Training with Existing Curriculum
Digital Prebriefing
Learners reviewed video content three to five days before the simulation.
In-Person Didactic Session
A 90-minute interactive lecture reinforced critical concepts necessary for recognizing and responding to open chest emergencies. The session focused on identifying the clinical signs of cardiac tamponade, reviewing the appropriate steps in the pulseless electrical activity (PEA) arrest algorithm, delineating each role within the open chest protocol, and reviewing the procedural steps of an emergency resternotomy.
Simulation Scenario
Simulation sessions were conducted in a dedicated, hospital-based simulation center designed to replicate a CVICU patient room, including monitoring equipment, emergency carts, and institutional open chest protocols. Teams engaged in a full-code scenario that progressed into an open chest emergency using the high-fidelity manikin. Briefly, the simulation began with staff recognizing clinical signs consistent with cardiac tamponade, including hypotension and narrow pulse pressure. This led to a PEA arrest, prompting the team to initiate open chest protocol and transition from standard CPR to sterile compressions. Staff were then expected to appropriately prep and drape the patient for resternotomy (Dunning et al., 2017).
During the simulation, learners were then required to incise the skin layer with a scalpel, cut through the simulated sternal wires, and use the sternal retractor to fully open the chest—ultimately exposing the silicone heart. This approach aimed to provide hands-on experience with each step of an emergency resternotomy. The design was informed by best practices in simulation fidelity (Hill et al., 2023) and existing emergency resternotomy protocols (Tsiouris et al., 2024).
Debriefing
Facilitators guided a reflective discussion focused on role clarity, procedural accuracy, and emotional response. Simulation recordings were professionally edited into single-session review videos and shared with learners, along with educator annotations, post-simulation to support continuous learning and reflective practice (Figure 1). After reviewing the recording, each attendee was required to submit three things that went well in the simulation and three things that could be improved upon using the Data Entry section of Learning Space.
Evaluation of Revised Training
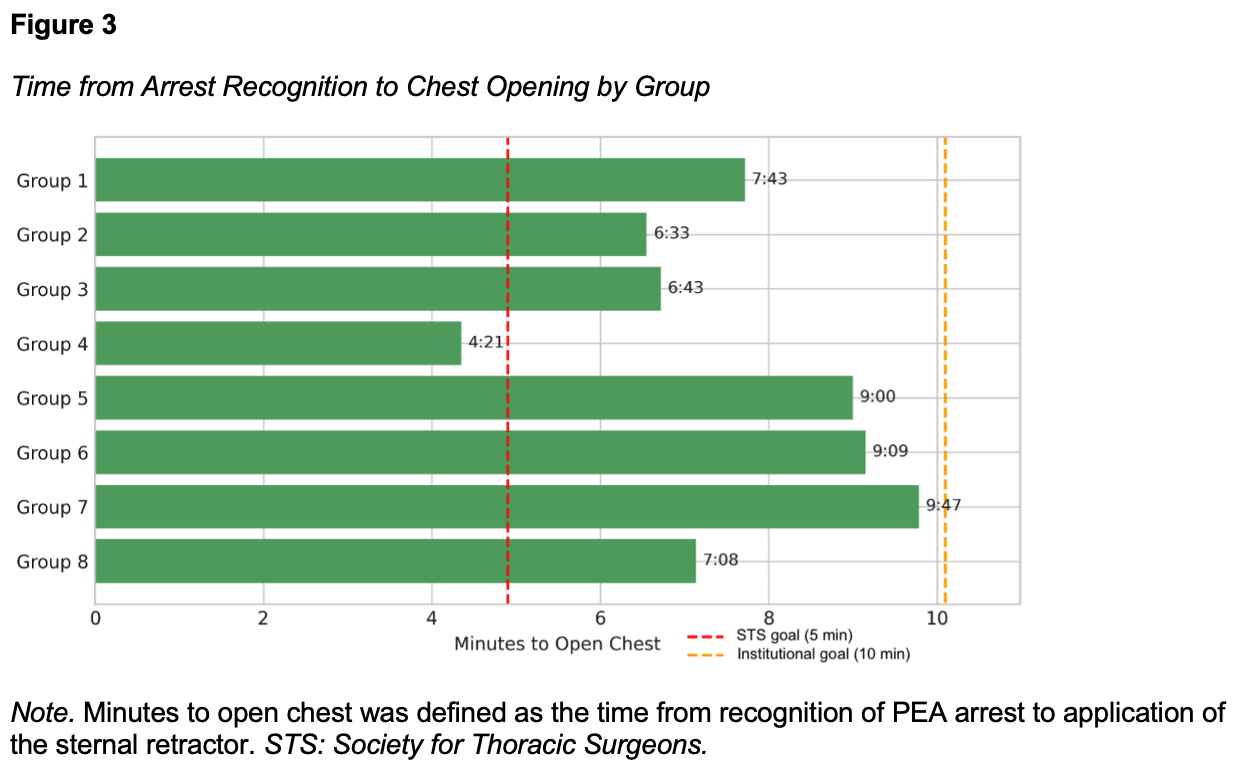
To evaluate the revised training, we looked at several metrics. The efficacy of the digital prebriefing was assessed using a two-question knowledge check prior to the start of the in-person didactic session. Correct responses on the knowledge check were compared between learners who received digital prebriefing and those who did not. In addition, each simulation session was recorded using multiple cameras from the simulation center. These recordings were reviewed in Learning Space to obtain time to chest opening, defined as the application of the sternal retractor, once PEA arrest was recognized. The time to chest opening was compared to the Society for Thoracic Surgeon goal of 5 minutes and the institutional goal of 10 minutes (Dunning et al., 2017). Qualitative feedback on the new simulation design was collected through open-ended post-activity survey questions. No survey response was excluded from analysis.
RESULTS
The initial implementation of this enhanced training in 2025 involved 41 learners – 36 registered nurses and 5 advanced practice providers. The learners were divided into 8 groups of 5 to 7 nurses and at least one advanced practice provider to complete the high-fidelity open chest simulation.
Knowledge Check
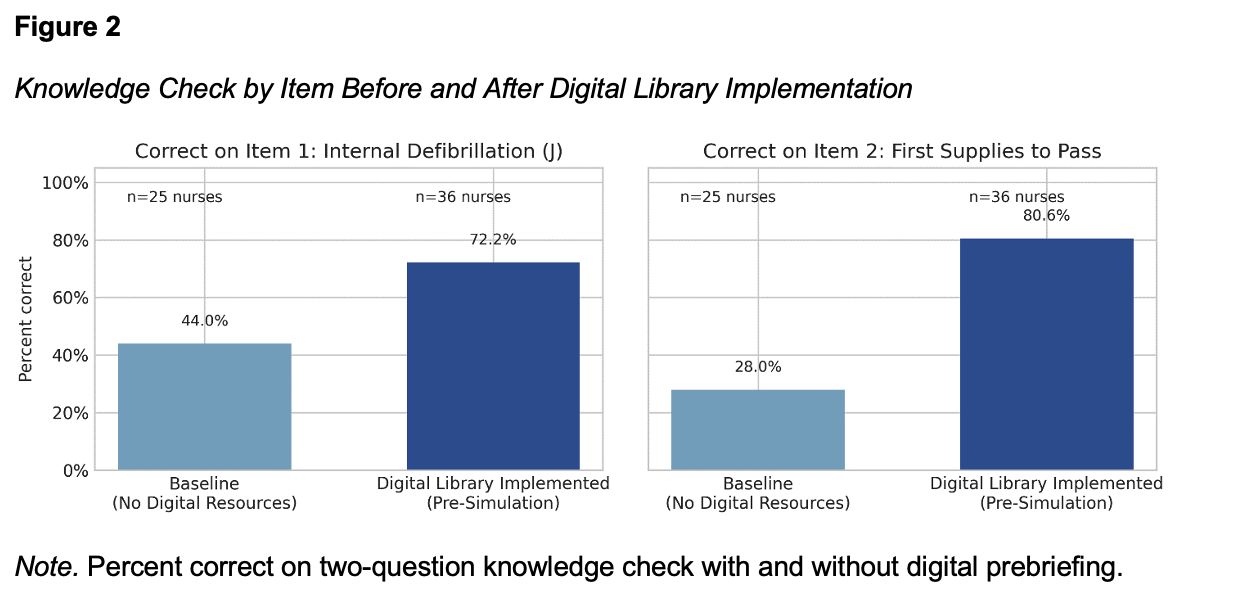
The two-question knowledge check prior to in-person didactics demonstrated the impact of digital prebriefing (Figure 2). For internal defibrillation in an open chest scenario, 72.2% of nurses correctly identified 20 joules as the appropriate charge with digital prebriefing, compared to 44.0% without. Similarly, 80.6% of nurses with digital debriefing correctly identified the open chest tray and scalpel as the first supplies to hand to a provider, compared to 28.0% without.
Time to Chest Opening
The time from recognizing PEA to successful chest opening varied considerably, ranging from four minutes and twenty-one seconds to nine minutes and forty-seven seconds (Figure 3). One group achieved chest reopening within the Society of Thoracic Surgeons’ recommended goal of five minutes (Dunning et al., 2017), while all groups met the institutional goal of ten minutes.
Learner Feedback
From the qualitative feedback collected after the simulation, comments reflected perceived improvements in preparedness, realism, and role clarity. A small number of learners identified opportunities for improvement, including requests for additional repetition and expanded role-specific practice time. Learners cited the value of digital preparation, enhanced realism of the manikin, and the usefulness of reviewing recorded simulation videos post-session. Simulation educators reported perceiving greater learner engagement and fewer interruptions during scenarios, attributing this to improved preparedness and equipment familiarity.
DISCUSSION
The combination of digital prebriefing and high-fidelity simulation addressed critical gaps in training by improving realism, repetition, and reflection. Learners exposed to the digital prebriefing had improved scores on knowledge checks before the simulation. This is reflected in their self-reported improved readiness and clearer understanding of responsibilities.
In previous iterations of open chest simulations at our institution, time to chest opening typically ranged from eight to ten minutes from arrest recognition, despite requiring fewer procedural steps. The improved times observed in this study suggest enhanced overall performance following implementation of the digital prebriefing and simulation redesign. This improvement may be partly attributed to the psychomotor learning facilitated by physically performing the chest opening with procedurally accurate tools and materials, compared to previous methods that lacked this hands-on component.
The post-simulation review videos allowed for ongoing reflection and the ability to identify improvement opportunities not recognized during live simulation. We have now expanded the use of our institution's Learning Space platform to further enhance the accessibility and customization of post-simulation content. This allows learners to extend the educational impact beyond the initial training day by revisiting recorded scenarios, debrief materials, and related reference videos.
Implementation of the enhanced open chest training program presented several logistical and resource‑related challenges. The development of a high‑fidelity thoracic cage required a substantial one‑time financial investment, estimated at approximately $60,000. This may present a barrier to adoption for institutions with limited simulation budgets. In addition, coordinating simulation sessions that included advanced practice providers was challenging due to competing clinical demands. Addressing these scheduling constraints required flexibility in session timing and strong collaboration with unit leadership to prioritize participation. Despite these challenges, this initial implementation suggests the educational benefits and improvements in team performance support continued use and expansion of the program.
Limitations
This initiative has several limitations. The post-activity survey relied primarily on self-reported confidence and perceptions rather than objective performance metrics. Additionally, the small sample size and single-center design limited generalizability. Future iterations will incorporate more robust assessment tools, including structured behavioral checklists and longitudinal follow-up to evaluate skill retention and clinical impact.
CONCLUSION
By integrating structured digital learning with high‑fidelity simulation, this initiative offers a practical and scalable approach to preparing CVICU teams for rare but life‑threatening open chest emergencies. The combination of role‑based pre‑work, anatomically realistic task training, and post‑simulation video review supported reported improved preparedness, procedural performance, and team engagement. While the model required initial resource investment and deliberate coordination, its design allows for adaptation across institutions and clinical contexts. Future efforts will focus on expanding this approach to additional high‑risk procedures and evaluating long‑term skill retention and translation to clinical practice.
REFERENCES
Dunning, J., Levine, A., Ley, J., Strang, T., Lizotte, D. E., Lamarche, Y., Bartley, T., Zellinger, M., Katz, N., Arora, R. C., Dembitsky, W., Cheng, A. M., Lonchyna, V. A., Haft, J., Deakin, C. D., Mitchell, J. D., Firestone, S., & Bakaeen, F. G. (2017). The Society of Thoracic Surgeons Expert Consensus for the resuscitation of patients who arrest after cardiac surgery. The Annals of Thoracic Surgery, 103(3), 1005–1020. https://doi.org/10.1016/j.athoracsur.2016.10.033
Hill, K., Schumann, M., Farren, L., & Clerkin, R. (2023). An evaluation of the use of Low-Fidelity and High-Fidelity mannequins in clinical simulations in a module preparing final year children’s and general nursing students for internship placement. Comprehensive Child and Adolescent Nursing, 46(4), 295–308. https://doi.org/10.1080/24694193.2023.2232456
Stewart, N., Gandhi, S., Krueger, A., & Chapman, B. (2024). 131: Visual Proficiency: Video-Driven ECMO Education in a Digital Age. ASAIO Journal, 70(Supplement 4), 110. https://doi.org/10.1097/01.mat.0001070504.51947.2c
Tsiouris, A., Protos, A. N., Keys, V. D., Chambers, D., Jeyakumar, A. K. C., & Shake, J. G. (2024). Simulation training for emergency sternotomy in the Cardiovascular Intensive Care Unit. Critical Care Nurse, 44(3), 12–18. https://doi.org/10.4037/ccn2024195