Examining the Use of a Digital Stethoscope within an Academic Medical Center Nursing Program
Authors
Joseph W. Tacy, Ph.D., RN1; Alaina Herrington, DNP, RN, FAAN, FSSH, ANEF, CHSE-A, CNOR(E)1; James Hughes, MD, FACS2; Masoumeh Karimi, PhD., MPH1; Robyn MacSorley, PhD, RN, CHSE1; Sharon McElwain, DNP, RN, FNP-BC1; Daniel Weiss, MD, FACS, BSEE2; Lei Zhang, PhD, MBA1
1University of Mississippi Medical Center, School of Nursing, Jackson, Mississippi
2Bongiovi Medical & Health Technologies, Port Saint Lucie, Florida
Conflict of Interest Statement
Dr. Weiss is the Chief Medical Officer of Bongiovi Medical and Dr. Hughes is the Medical Director of Bongiovi Medical. This study utilized a stethoscope that is a product of Bongiovi Medical.
Corresponding Author
Joseph W. Tacy, Ph.D., RN, University of Mississippi Medical Center School of Nursing, Jackson, Mississippi
Email: jtacy@umc.edu
Brief Description
The conventional method of auscultation has not progressed alongside the introduction of new technologies. With the advent of computer-aided audio enhancement, healthcare professionals now have the ability to listen to amplified sound waves. However, it remains uncertain whether this enhancement can improve skill levels and offer the same ease of use as traditional stethoscopes. This study aimed to compare the effectiveness of an analog stethoscope with intelligent auscultation technology in clinical diagnosis and the training of nursing students. The results revealed that electronic digital stethoscopes deliver enhanced sound compared to the traditional method, potentially advancing educational practices and disease diagnosis in the field.
Introduction
Auscultation is one of the basic techniques for diagnosing heart, lung, and bowel abnormality and normality. However, the interpretation of sounds is a subjective and difficult skill to develop with significant inter-listener variability (Kevat, Kalirajah, & Roseby, 2020). Computer-aided audio enhancement (making relevant diagnostic sounds more audible to the human ear) and detection technology (using Artificial Intelligence [AI], to help make the diagnosis) are fast and efficient instruments for the use of quantitative acquisition and the analysis of sound signals. Currently, intelligent auscultation technology has not been widely used in clinical diagnosis and training (Li et al., 2020). The current primary method used for auscultating sound detection is manual stethoscope auscultation. Therefore, the research and application of computer-aided techniques for sound detection will promote development in the field of education and disease diagnosis.
In this study, nursing students at an academic medical center observed and compared an analog stethoscope with two different electronic stethoscopes (Figures 1 and 2) to determine if there is a significant difference in the diagnostic utility of each device. Further analysis was completed to examine if perceived usefulness, perceived ease of use, attitude toward using, and behavioral intent to use the electronic digital stethoscope showed variation in actual use.
Background
Stethoscopes have been widely utilized in medical and healthcare education since its introduction in 1816 by Rene Laennec, which consisted of a monoaural wooden tube (Silverman & Bulk, 2019). In 1840 a flexible tube was introduced, and then by 1852 a binaural stethoscope was developed and brought to the commercial market. The design has not significantly changed with present-day stethoscopes, with the most popular ones either being a Littmann or Sprague design with improved materials (Silverman & Bulk, 2019). The traditional stethoscope design operates via a disc-shaped resonator that is placed upon the body will transmit sound through a hollow air-filled tube to the listener’s ears. Electronic stethoscopes were first introduced in the 1950s but did not enter the clinical field until the mid-1990s when 3M introduced their model (Leng et al., 2015). This new model provided the ability to amplify and convert sound waves into electrical signals that were processed and produced for enhanced listening. However, this new form of electronic listening led to amplified artifacts and sound alteration due to conduction thresholds which led some to question whether this was an improvement. Some in the healthcare industry have called the current stethoscope a “relic”, noting that other devices that connect to smartphones can amplify heartbeats, help with diagnosis, and the data can be sent wirelessly to patients’ electronic medical records (Taylor, n.d.). Current advances in technology seem impressive, and its impact on healthcare practice is heading down the high-tech superhighway.
With the prevalence of unhealthy living habits, adverse acute and chronic disease has become one of the major risks to human health. The health disadvantage is pervasive, affecting all age groups, and is witnessed in multiple diseases, biological and behavioral risk factors, and injuries (NRC, 2013). Most heart and lung diseases are associated with and reflected by the sounds that the body organ produces. Auscultation, defined as listening to the resonance sound the body makes, whether it be heart, lung, or bowel sounds, historically is an important method for the early diagnosis of dysfunction (Cleveland Clinic, 2022). Traditional auscultation requires substantial clinical experience and competent listening skills. As a result of the electronic stethoscope, a new field of computer-aided auscultation has emerged.
Methods
The aim of this study is to compare and contrast an analog stethoscope versus two digital stethoscopes in healthcare education among nursing students. This study utilized a quasi-experimental design implemented in two phases. The first phase utilizes classroom instruction and simulated sounds within the lab setting. The second phase of the study is to examine the devices within the clinical and telehealth setting. This article will focus on the first phase of the study.
Devices
The Aria Stethoscope (Bongiovi Medical and Health Technologies) (Figure 1) is designed to be an integrated, high-quality, extended frequency range capture device for biological sounds. The Aria is supplemented by a Medical Device Power Station (MDPS), a proprietary audio signal-processing software solution that optimizes the sound for intelligibility during telemedicine and other extreme acoustic environments. The Aria stethoscope integrates with a mobile application that provides the MDPS processing as part of an audio loopback feature, as well as audio recording and note-taking. The mobile application enables easy integration into multiple systems, hardware, or environments. The Aria is also designed to function as a stand-alone auscultation instrument with proper hardware attachments. The Aria stethoscopes used in this study were three-dimensional (3D) printed prototypes, as this stethoscope has not yet entered mass production.
The M1 Telehealth Stethoscope (Medaica) (Figure 2) is a new stethoscope released in the low-cost tele-auscultation market. It has Food and Drug Administration (FDA) approval for home use and features a built-in digital interface for use with smartphones and computers, as well as a separate microphone for voice communication. The M1 also utilizes MDPS audio processing for sound optimization. In this study, the M1 stethoscope was used with the Aria mobile application and MDPS audio processing to standardize the student workflow for the electronic stethoscopes. The standard traditional stethoscope used was a Sprague type. All students were given this stethoscope to use as a participant in the study to reduce variability among their personal stethoscopes.
Figure 1: Aria Stethoscope

Figure 2: Medaica Stethoscope
Participants
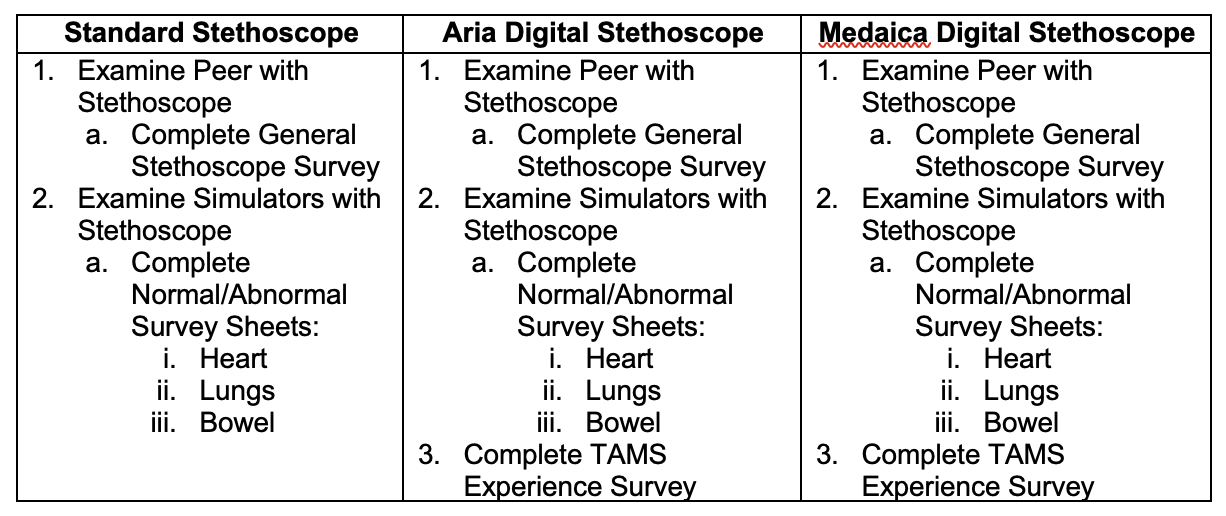
The classroom instructional phase of this study included 32 pre-licensure and 4 advanced practice nursing students. It was conducted between 06/01/2022 and 06/01/2023. The inclusion criteria for the study consisted of traditional and accelerated pre-licensure Bachelor of Science in Nursing (BSN), and advanced nursing students eligible to participate in the study if they provided consent. The study information flyer with a quick response (QR) code was hung up in the back of the classroom and disseminated via email and the learning management system email to solicit participants. Participants had the option to sign consent and enroll electronically by using the QR code link. Participation was on a first come, first serve basis per consent received. Participants received a $20 gift card to Walmart for their time. Participants were instructed on the use of all devices and provided surveys at the start of the session. Examination occurred with all 3 stethoscopes and subsequently completed the survey responses in order as outlined in Table 1.
Figure 3: Participant Procedure Process
Survey and Operational Definitions
The instructional classroom phase of the study utilized three survey instruments and a verbal qualitative debriefing activity. The general stethoscope survey, the Normal/Abnormal survey, and the technology acceptance survey. The general stethoscope survey consists of 12 questions that ascertain the quality and or clarity of sound while using all 3 stethoscopes to listen to the participant's heart, lung, and bowel sounds using a 7-point Likert scale. In addition to this, there was a question posed to assess and record a blood pressure reading using a manual cuff on a simulated arm. The Normal/Abnormal survey consists of ascertaining the quality of sound while using all 3 stethoscopes to listen to simulated heart and lung sounds via 3B Scientific Heart & Breath Sounds Simulator and bowel sounds via Gaumard Adult HAL simulator using a 7-point Likert scale.
The Technology Acceptance Model (TAM) was adapted to explicate the factors affecting technology use (Davis, 1989; Venkatesh & Davis, 2000). Davis’s model postulates that technology usage is determined by two leading beliefs, perceived usefulness, and perceived ease of use. Attitude towards use and behavioral intention to use technology will affect how individuals respond to technology; therefore, attitude and behavior is inferred to partially impact the effect of perceived ease of use and perceived usefulness on actual use of technology.
Participants utilized the TAM scale to rate both digital stethoscopes during the classroom/lab instruction and is based on 5 sub-scales in a 7-point-Likert type format defined here. Perceived usefulness (PU) is defined as the degree to which an individual believes that using a particular technology will enhance job performance (Davis, 1989). Perceived ease of use (PEU) is considered the extent to which an individual believes that using technology/system would be free of effort (Venkatesh et al., 2008). Attitude toward using (AT) is defined as an individual's positive or negative feelings about performing the target behavior. Attitude toward using electronic learning will be measured using Mishra and Panda’s Attitude Toward E-learning (ATEL) scale (Mishra & Panda, 2007). Seven statements on the ATEL are negatively worded and thus will be reversed scored. Behavioral intent to use (BI) is the degree to which a person has formulated conscious plans to perform or not perform some specified future behavior (Venkatesh et al., 2008; Kim, Chun, & Song, 2009).
Data Analysis
The data were imported from REDCap to IBM Statistical Package for the Social Science (SPSS) 28.0 for analysis. One-way Analysis of Variance (ANOVA) was used to compare the mean responses from the three different devices. Independent sample t-test was conducted to compare the result of the survey between the two digital devices. The linear regression model was used to investigate factors associated with the actual use intention given that the participant has access to either one of the devices. All statistical tests were two-sided. Level of significance (alpha) was set at 0.05. P<0.05 from ANOVA or linear regression shows a significant difference in means or indicates a significant factor for certain outcome measures.
Results
Qualitative
Verbal feedback gained during the debriefing session with students varied greatly. Overall, the participants expressed the inability to hear well with the standard stethoscope used in the study. The students were comfortable with the use of the stethoscope and felt it was easy to carry and could be quickly accessed for use. Students had mixed feedback on which digital stethoscope they preferred, primarily most students enjoyed the Aria. Multiple students reported that the Aria was able to provide the sound they were trying to hear while reducing other environmental artifacts. They did not have any prior knowledge of the device and its ability to perform this function, but they were able to detect this. Others preferred the Mediaca stating it picked up all sounds and they could hear everything, which gave them the confidence to identify the sounds they were attempting to hear. This is something health care professionals are familiar with standard stethoscopes and could be the rationale for this. All students felt the sound of the digital devices were far superior to that of the standard Sprague but in terms of utility, the Sprague was the easiest to use. The Mediaca was also identified as slightly easier to due to the handlebar like design, but students equally agreed that this design could create difficulties depending on where you were listening.
Quantitative
Comparing the three stethoscope survey results, showed slightly higher preference rate for Aria compared to the other 2 devices but the differences were not statistically significant. This result is similar to the qualitative results stated above. Within the general stethoscope survey, students measured a standardized blood pressure of 120/80 on a simulated arm using all 3 stethoscopes. In all 3 devices, the average recorded systolic BP was lower than 120 mmHg and diastolic BP was higher than 80 mmHg set values. Among all 3 stethoscopes, there were no significant findings based on the survey results in variation of measured blood pressure. The only statistically significant difference among devices was with the performance of a manual blood pressure assessment with manual cuff (F(2,87) = 8.33, p < 0.001). A Bonferroni post hoc test revealed that it is significantly easier to use Sprague stethoscope (mean= 6.10, SD=0.9) compared to Aria (mean= 4.36, SD=2.28) and M1 (mean= 4.61, SD=1.94) stethoscopes to obtain a result from a manual cuff.
Using the Normal/Abnormal survey, students rated the quality of the heart, lung and bowel sound. The overall result showed that students rated the digital stethoscopes higher than the analog one. The summary of the analysis is provided in Table 2.
Table 2: Comparing the rates of the 3 stethoscopes in sound quality.
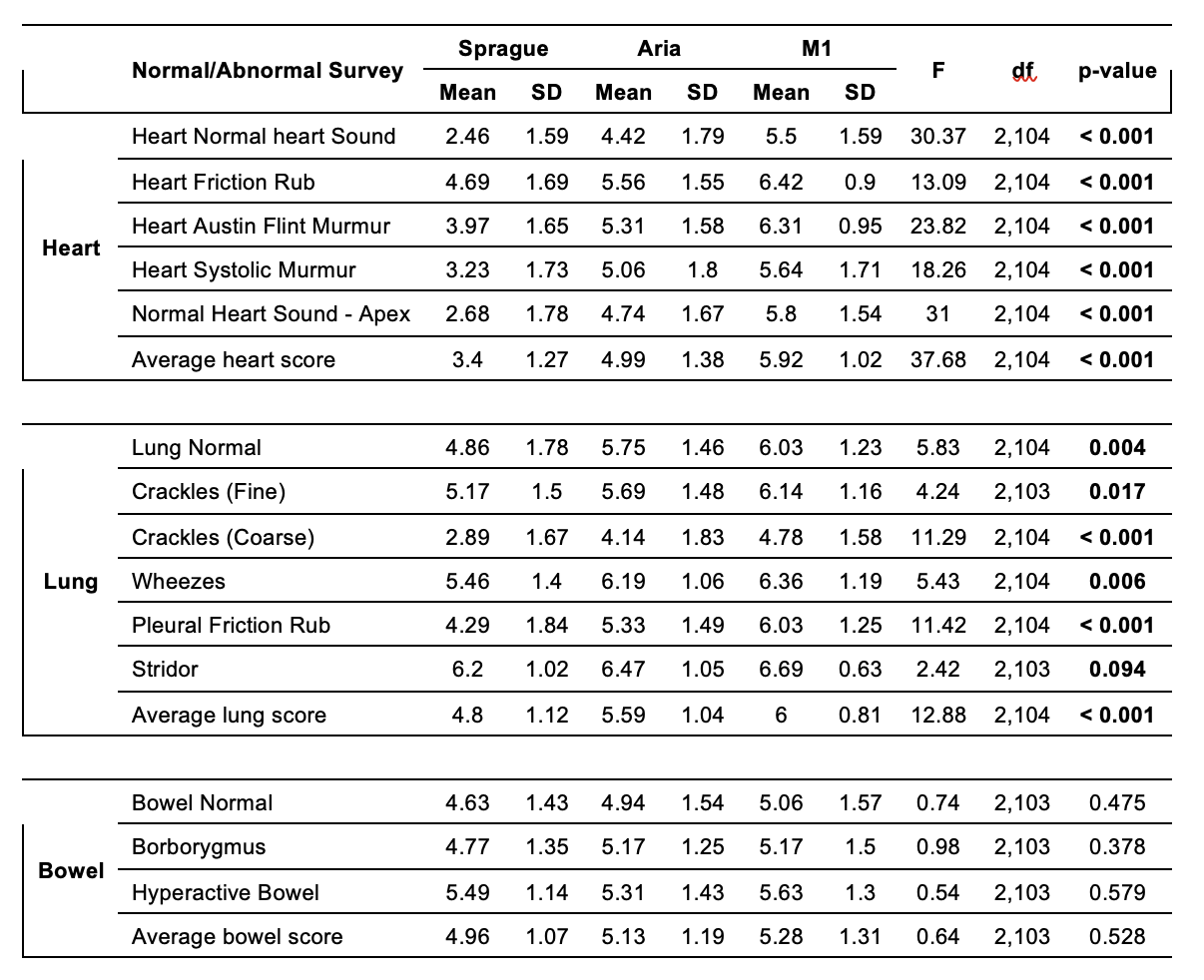
According to Table 2, there was a statistically significant difference in the quality of heart sound between devices (F(2,104) = 37.68, p < 0.001). A Bonferroni post hoc test revealed that while listening to heart sound, M1 (mean= 5.92, SD=1.02) stethoscope rates the most excellent one, followed by Aria (mean= 4.99, SD=1.38), and Sprague stethoscope rates the poorest (mean= 3.4, SD=1.27). The same results were found rating the lung sound quality (ANOVA (F(2,104) = 12.88, p < 0.001). A Bonferroni post hoc test revealed that M1 (mean= 6.0, SD=0.81) stethoscope rates the most excellent one, followed by Aria (mean= 5.59, SD=1.04); And Sprague stethoscope rates the poorest (mean= 4.8, SD=1.12). Although the participants rated M1 (Mean= 5.3, SD= 1.31) and Aria (Mean= 5.1, SD= 1.19) higher than Sprague (Mean= 4.9, SD= 1.07) stethoscopes in bowel sound quality, the differences were not statistically significant (F(2,103)= 0.64, p=0.528).
Utilizing the Technology Acceptance Model, this study intended to examine the use of digital stethoscopes. The result of the Independent Sample t-test didn’t show any significant difference in TAM items rating between the 2 digital stethoscopes. A linear regression analysis performed on TAM average score of the “Actual Use” item in Aria and M1 stethoscopes to find the significant predictor of the actual use intention given that the participant has access to either one of the devices.
Table 3: Linear regression analysis of TAM.
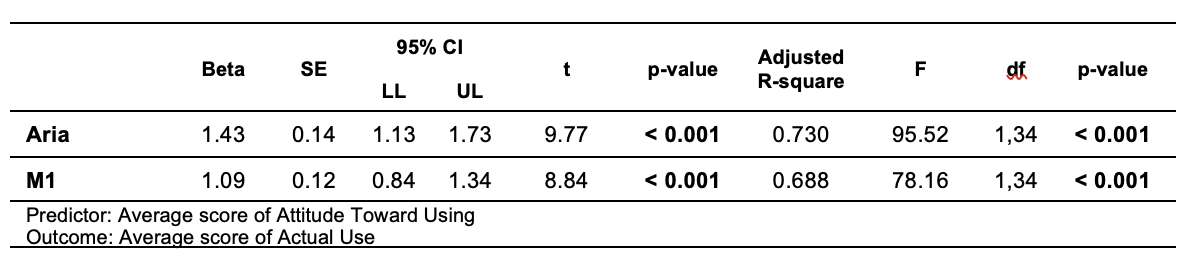
The result of both linear regression models (Table 3) found “attitude toward using” being the only significant predictor of “actual use” of both Aria and M1 stethoscopes. The higher the attitude score, the higher the possibility of “actual use” (Aria: b=1.43, t=9.77, p < 0.001; M1:b=1.09, t=8.84, p < 0.001).
Discussion
Studies over time have found the stethoscope to be a valuable diagnostic instrument in the daily use of health assessment (Silverman & Balk, 2019). Unlike traditional stethoscopes based on the physics of sound movement via a diaphragm and air-chambered tube, digital stethoscopes can provide enhanced sound with cutting-edge AI-infused technology. Both Aria and M1 utilize the same technology to listen to enhanced sound movement, with the Aria having the ability to compensate to remove artificial artifact when compared to other devices. This result could be related to the feedback that the students were more comfortable hearing all the surrounding artifacts given that is how they were trained using a standard stethoscope and were comfortable learning by this method. If they knew the original intent of the device to assist by isolating the sound they were attempting to hear, this could have created a different viewpoint and resultant outcome. As noted above in the qualitative results, some students did ascertain this from the use.
Various weaknesses/limitations were discovered during the deployment of this study. One unexpected issue was the rate at which student participation was anticipated. 32 out of 270 pre-licensure students agreed to participate in this study, which represents a 12% participation rate. Four out of 100 advanced practice students also participated, which represents a 0.04% participation rate. This was an unexpectedly low response rate from students to volunteer in the study. The original intent was to pay all study participants at the end of the phases of the study, this had to be altered during phase 1 participant data collection. Due to very low volunteer enrollment, the Institutional Review Board (IRB) was modified to permit payment at the end of each phase, which did increase participant enrollment by 44%. Future scholarly endeavors in the realm of teaching and learning would benefit from the alignment of studies within course delivery to garner higher participation. Another weakness was the prototype nature of the devices used, the prototypes sometimes would have interference and feedback that required interruption by the PI to troubleshoot the devices to achieve the required use of the device through corrective adjustments.
Conclusion
In this study, the latest technology-aided audio detection technologies were utilized to provide enhanced sound compared to the traditional diagnostic modalities to promote development in the field of education and disease diagnosis. Results from this study validated the performance, quality, and generalizability for the use of a digital stethoscope utilizing a mobile application that provides the MDPS processing for audio presentation within healthcare education. Further studies are required to explore functionality, design, and applicability of these prototypes in alternate settings. This study manuscript represents the completion of the first phase of the project. The next phase of this study will be performed to examine the use of the digital stethoscope within the clinical and telehealth training environments.
References
Cleveland Clinic. (2022). Auscultation. https://my.clevelandclinic.org/health/diagnostics/23080-auscultation#:~:text=The%20medical%20definition%20of%20auscultation,the%20sounds%20of%20your%20body
Davis, F.D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. Mis Quarterly, 13(3), 319-340.
Kevat, A., Kalirajah, A., & Roseby, R. (2020). Artificial intelligence accuracy in detecting pathological breath sounds in children using digital stethoscopes. Respiratory research, 21(1), 253. https://doi.org/10.1186/s12931-020-01523-9 https://doi.org/10.1186/s12931-020-01523-9
Kim, Y.J., Chun, J.U., & Song, J. (2009) Investigating the role of attitude in technology acceptance from an attitude strength perspective. International Journal of Information Management, 29(1), 67-77. doi:10.1016/j.ijinfomgt.2008.01.011
Leng, S., Tan, R. S., Chai, K. T., Wang, C., Ghista, D., & Zhong, L. (2015). The electronic stethoscope. Biomedical engineering online, 14, 66. https://doi.org/10.1186/s12938-015-0056-y
Li, S., Li, F., Tang, S., & Xiong, W. (2020). A Review of Computer-Aided Heart Sound Detection Techniques. BioMed research international, 2020, 5846191. https://doi.org/10.1155/2020/5846191
Mishra, S. & Panda, S. (2007). E-learning in a mega open university: Faculty attitude, barriers, and motivators. Educational Media International,44(4), 323-338.
National Research Council (NRC) (US), Institute of Medicine (US), Woolf, S. H., & Aron, L. (Eds.). (2013). U.S. Health in International Perspective: Shorter Lives, Poorer Health. National Academies Press (US).
Silverman, B., & Balk, M. (2019). Digital Stethoscope-Improved Auscultation at the Bedside. The American journal of cardiology, 123(6), 984–985. https://doi.org/10.1016/j.amjcard.2018.12.022
Taylor, P. (n.d.) Why are doctors still using the stethoscope? Health Debate https://healthydebate.ca/2016/02/topic/are-stethoscopes-passe/
Venkatesh, V. & Davis, F. (2000) A theoretical extension of the technology acceptance model: four longitudinal field studies. Management Science, 46(2), 186-204. https://doi.org/10.1287/mnsc.46.2.186.11926
Venkatesh, V., Brown, S.A., Maruping, L.M., & Bala, H. (2008). Predicting different conceptualizations of system use: The competing roles of behavioral intention, facilitating conditions, and behavioral expectation. MIS Quarterly, 32(3), 483–502. https://doi.org/10.2307/25148853